Main Tab |
  
|
Main Tab |
|
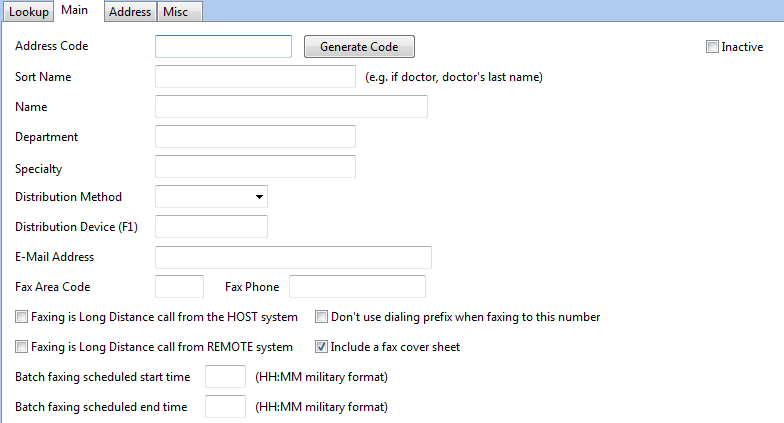
ADDRESS CODE: Key in a unique numeric or alphanumeric code, or select Generate Code
SORT NAME: Generally the last name of the provider
NAME: Full name - First M Last, credentials (John S Smith, MD)
DEPARTMENT: If applicable. This field is for informational purposes only
SPECIALITY: If applicable. This field is for informational purposes only
DISTRIBUTION METHOD:
NONE - No distribution
FAX - Fax distribution
EMAIL - Email distribution
PRINT - Automatic printing of cc's to a printer configured in the sites' Device setup
WEBPORTAL - Provider will review documents via the web portal.
DEVICE: Copies will distribute to a device configured in the sites' Device setup
DISTRIBUTION DEVICE (F1): Devices define how transcribed documents will be distributed to the end user. This is in addition to the Forms Distribution if this address is used as a CC.
EMAIL ADDRESS: If the distribution method is EMAIL, enter the provider's email address.
NOTE: This is not a secure method of sending documents and should not be used for documents containing private information or protected health information.
FAX AREA CODE: If the distribution method is FAX, enter the fax area code
FAX PHONE: If the distribution method is FAX, enter the fax phone number
FAXING IS LONG DISTANCE CALL FROM THE HOST: If faxing is done by your server, use Y if you need to dial an area code for the fax number..
FAXING IS LONG DISTANCE CALL FROM REMOTE: If faxing is being done by a remote server, use Y if you need to dial an area code for the fax number.
BATCH FAXING SCHEDULED START AND END TIME: If the provider only wants to receive faxes at certain times, enter the start and end time in HH:MM format.